

Notes
1
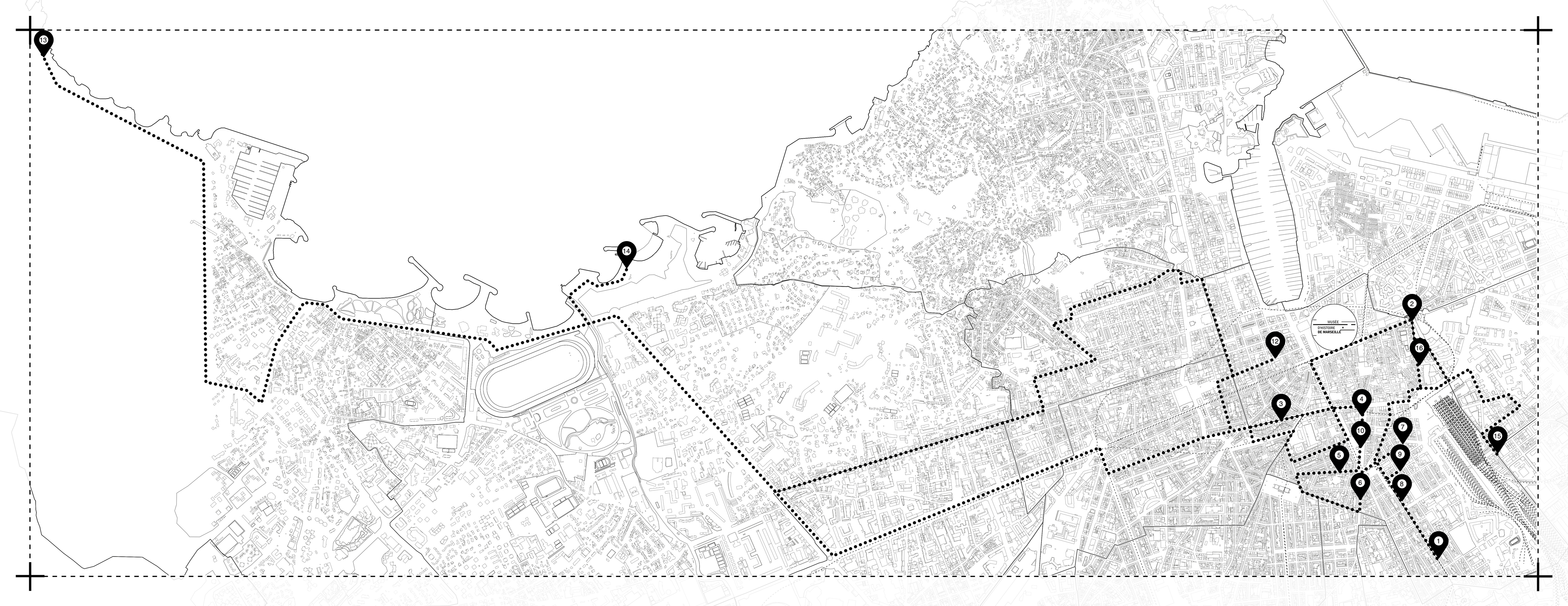
The voices of these oral histories constituted the main body of the exhibition Housing Pharmacology at the Musée d’Histoire de Marseille conceived for the occasion of Manifesta 13, Marseille 2020.
2
The SIAO is a platform in each Département for the coordination and regulation of the hospitality, accommodation, and support sectors to assist in the integration and housing of homeless people.
© 2020 e-flux and the author